Safety Rate
Starting a family is one of the most personal journeys a woman can take. When that journey becomes difficult, it helps to understand what is happening inside your body — not in confusing medical language, but in plain words that actually make sense.
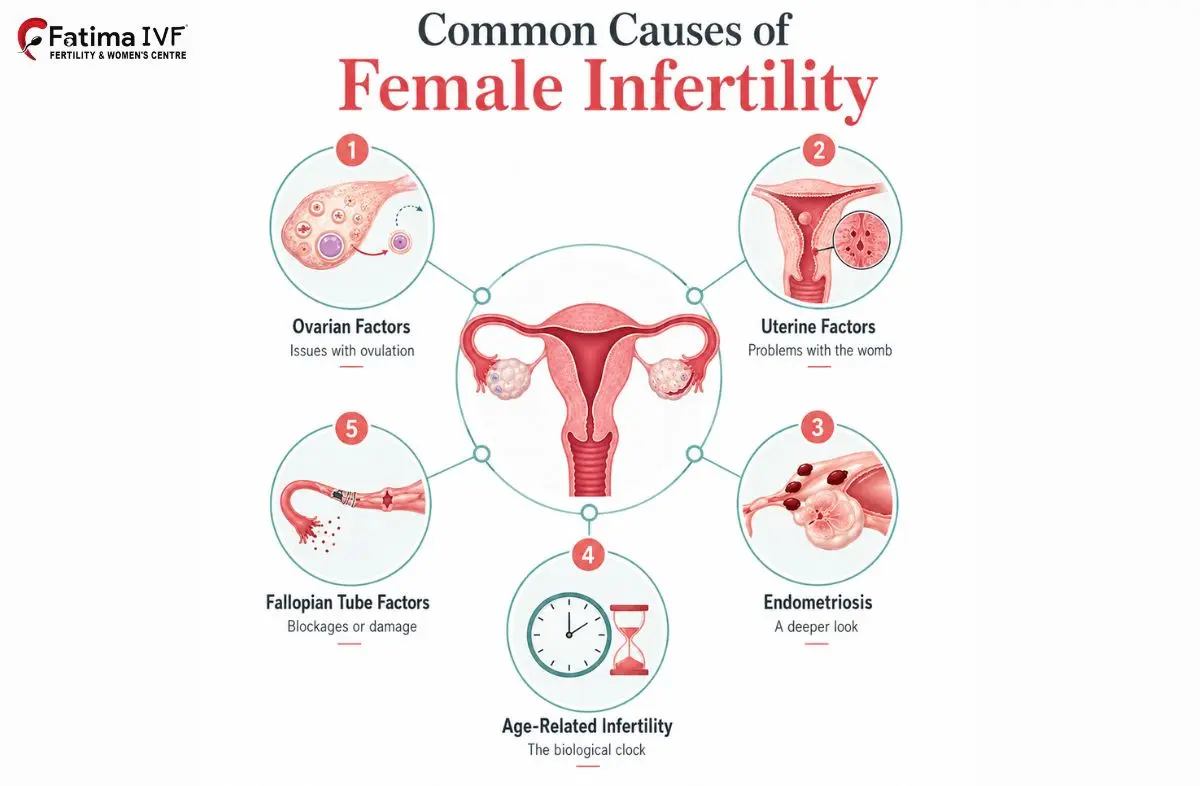
Female infertility conditions cover a wide range of health issues that can make it harder to get pregnant or carry a pregnancy to full term. Some conditions are structural, meaning they affect the shape or function of the uterus or fallopian tubes. Others are hormonal, affecting the way your body produces or responds to reproductive hormones. A few are related to recurring infections or immune responses.
The good news is that most female infertility conditions are treatable. Early diagnosis makes a real difference. At Fatima Fertility Centre, Chennai, Dr. Fathimunissa brings years of dedicated experience in diagnosing and managing these conditions with care and compassion. She believes that every woman deserves a thorough explanation of her health — not just a prescription.
This page walks you through each condition clearly, covering what it is, how it affects fertility, and what treatment options look like. Whether you are just beginning to explore or have already received a diagnosis, this guide is here to help you move forward with confidence.
A uterine septum is a wall of tissue that divides the inside of the uterus into two separate sections. This wall, called a septum, forms during fetal development when the two halves of the uterus do not fully merge and the tissue between them does not dissolve as it should. It is actually one of the most common structural abnormalities of the uterus found in women.
The septum itself has a poor blood supply compared to normal uterine tissue. When an embryo implants on or near the septum, it may not receive adequate blood flow and nutrients. This increases the risk of miscarriage, particularly in the first trimester. Some women with a uterine septum may also experience preterm labour, abnormal positioning of the baby, or difficulty conceiving in the first place. Many women have no symptoms and only discover the septum after investigating repeated pregnancy losses.
The standard treatment is a minor surgical procedure called hysteroscopic septoplasty. A thin camera (hysteroscope) is passed through the cervix and into the uterus without any external cuts. The septum is then carefully divided using fine surgical instruments. The procedure is done under general or local anaesthesia as a day case — most women go home the same day. Recovery is quick, and pregnancy outcomes typically improve significantly after the septum is removed. Dr. Fathimunissa assesses each case with ultrasound and hysteroscopy to confirm the diagnosis before planning treatment.
Uterine scars, also known as intrauterine adhesions or Asherman's Syndrome, are bands of scar tissue that form inside the uterine cavity. These adhesions stick the walls of the uterus together — sometimes partially, sometimes extensively — reducing the space available for an embryo to grow.
Scar tissue inside the uterus disrupts the normal uterine lining (endometrium). When the lining cannot grow properly, it becomes difficult for a fertilised egg to implant and develop. Women with significant adhesions may experience lighter-than-normal periods, absent periods, or pelvic cramping. In more severe cases, the uterine cavity may be almost entirely blocked, making natural conception very unlikely.
Treatment involves hysteroscopic adhesiolysis — a procedure where the adhesions are carefully cut and removed using a hysteroscope. After the procedure, a thin balloon or an intrauterine device may be placed temporarily inside the uterus to keep the walls from sticking back together while healing takes place. Hormonal treatment is often prescribed alongside surgery to help rebuild the uterine lining. Regular follow-up with ultrasound or repeat hysteroscopy confirms whether the cavity has healed well. Results are generally positive, especially when the adhesions are detected and treated early.
Fibroids are non-cancerous (benign) growths that develop in or around the uterus. They are made up of muscle and fibrous tissue and can vary enormously in size — from as small as a seed to as large as a grapefruit. Fibroids are quite common, particularly in women in their 30s and 40s.
Not all fibroids cause fertility problems. The location of the fibroid matters more than the size. Fibroids that grow inside the uterine cavity (submucosal fibroids) are the most likely to affect fertility because they distort the space where an embryo needs to implant. They can also alter blood flow to the uterine lining. Fibroids in the wall of the uterus (intramural) may cause problems if they are large enough to press on the cavity. Fibroids on the outer surface (subserosal) rarely affect fertility directly. Symptoms include heavy periods, pelvic pressure, frequent urination, and lower back pain — though many women have no symptoms at all.
Treatment depends on the size, number, and location of the fibroids, as well as the woman's plans for pregnancy. Small fibroids with no symptoms may not require treatment — just monitoring. Submucosal fibroids are best removed hysteroscopically, while larger intramural fibroids may require laparoscopic or open myomectomy (surgical removal of the fibroids while preserving the uterus). Dr. Fathimunissa discusses each case individually to determine whether fibroid removal is needed before attempting conception and which approach is safest and most effective.
Uterine polyps are small, soft growths attached to the inner lining of the uterus. They develop when the endometrial tissue overgrows in a localised area, forming a finger-like or rounded projection into the uterine cavity. Polyps are usually benign, but they can interfere with fertility.
Polyps may block the fallopian tube openings, preventing sperm from reaching the egg. They can also disrupt the uterine environment in ways that make it harder for an embryo to implant. Women with polyps may experience irregular bleeding, spotting between periods, or bleeding after intercourse. Some women have no symptoms and only discover polyps during an ultrasound or hysteroscopy investigation for infertility.
Polyps are removed during a hysteroscopy procedure. The polyp is located using the camera and then carefully removed using small instruments. The procedure is usually quick and well-tolerated. After removal, the uterine lining regenerates naturally. Many women find that their periods become more regular and their fertility improves after polypectomy. Removed tissue is always sent for laboratory examination to rule out any unusual cell changes.
Menstrual disorders refer to any significant deviation from a regular, healthy menstrual cycle. A normal cycle lasts between 21 and 35 days, with bleeding lasting three to seven days. Cycles that are too short, too long, too heavy, too light, very painful, or absent can all signal an underlying issue that may affect fertility.
The menstrual cycle is a direct reflection of the reproductive system's health. When cycles are irregular or absent, ovulation may not be occurring reliably — or at all. Without regular ovulation, natural conception becomes much harder. Heavy or painful periods can be a sign of conditions like endometriosis or fibroids that themselves affect fertility. Identifying the cause of the menstrual disorder is the first step toward restoring fertility.
Treatment is directed at the underlying cause. Hormonal therapies can regulate the cycle. Thyroid disorders require specific medication. Lifestyle changes — including reaching a healthy body weight, managing stress, and adjusting exercise intensity — can restore regular cycles in many women. Conditions like PCOS, fibroids, or endometriosis require their own targeted treatment, which is covered in the relevant sections below. Dr. Fathimunissa takes a thorough history and runs appropriate investigations before recommending any treatment.
Ovarian reserve refers to the number and quality of eggs remaining in the ovaries. Every woman is born with a fixed number of eggs, and that number naturally declines with age. Low ovarian reserve means fewer eggs are available than expected for a woman's age.
A reduced number of eggs means fewer chances per cycle for fertilisation. Even if the eggs that remain are of good quality, there are fewer opportunities. Women with low ovarian reserve may respond less well to ovarian stimulation during IVF cycles, producing fewer eggs for collection. This can make treatment more challenging and may require adjusted protocols. The quality of the remaining eggs also tends to decline with age, which affects the likelihood of a healthy pregnancy.
Testing ovarian reserve involves a combination of blood tests (AMH — anti-Müllerian hormone, and FSH) along with an antral follicle count done on ultrasound. These give Dr. Fathimunissa a clear picture of where your reserve stands. For women with mildly reduced reserve, natural timed intercourse with monitoring or IUI may still be effective. For those with significantly reduced reserve, IVF with tailored stimulation protocols maximises the number of eggs retrieved. In some cases, donor eggs may be discussed as an option. Early testing is valuable — the sooner a woman knows her reserve level, the more choices she has available.
Polycystic Ovarian Syndrome is one of the most common female infertility conditions seen in reproductive-age women. It is a hormonal condition where the ovaries produce higher-than-normal levels of androgens (male-type hormones), which interferes with the development and release of eggs.
In PCOS, the follicles in the ovaries start to grow but do not mature fully and do not release an egg — a process called anovulation. Without regular ovulation, pregnancy cannot occur naturally. Women with PCOS also have a higher risk of insulin resistance, which further disrupts hormonal balance. Long-term, unmanaged PCOS increases the risk of type 2 diabetes and cardiovascular issues.
Treatment is tailored to the individual's goals. For women trying to conceive, lifestyle changes — particularly weight loss of even 5–10% in women who are overweight — can restore ovulation naturally. Medications like Clomiphene or Letrozole are commonly used to stimulate ovulation. Metformin (an insulin-sensitising medication) is often prescribed alongside. If these measures do not result in pregnancy, IUI or IVF may be recommended. A procedure called laparoscopic ovarian drilling can also be offered in selected cases to restore ovulation. Dr. Fathimunissa provides a clear, step-by-step plan based on each woman's PCOS profile.
PCOD (Polycystic Ovarian Disease) and PCOS are closely related but not identical. In PCOD, the ovaries release immature or partially mature eggs, which accumulate as cysts. The condition is generally considered a milder form than PCOS, and the ovaries remain capable of functioning — but not at their full potential.
Women with PCOD often still ovulate, but erratically. This makes natural conception possible but unpredictable. Irregular periods, mild hormonal imbalance, and weight fluctuations are common. If left unmanaged, PCOD can progress or make conception consistently difficult. It is also associated with hormonal symptoms similar to PCOS, though generally less severe.
Lifestyle management is the cornerstone of PCOD treatment. A balanced diet, regular physical activity, and maintaining a healthy weight can significantly normalise the cycle and improve hormonal balance. Where periods remain irregular despite lifestyle changes, hormonal support or ovulation induction with low-dose medication may be recommended. Regular monitoring ensures that any deterioration is caught early and managed appropriately.
The fallopian tubes are two narrow passages that connect the ovaries to the uterus. After ovulation, the egg travels down a fallopian tube to meet sperm. Fertilisation normally takes place inside the tube. If the tubes are damaged or blocked, sperm and egg cannot meet, and natural pregnancy cannot occur.
Even if only one tube is blocked, fertility is reduced because only one tube is available each cycle. With both tubes blocked, natural conception is not possible, and IVF is typically required. Hydrosalpinx is particularly important in the context of IVF because fluid leaking back from the tube into the uterus can affect embryo implantation rates. Tubal disorders are responsible for a significant proportion of female infertility conditions investigated at fertility clinics.
A procedure called a hysterosalpingogram (HSG) is commonly used to check whether the tubes are open. Laparoscopy with dye testing provides more detailed information. Where possible, blocked tubes may be opened surgically. Hydrosalpinx tubes are often removed or clipped laparoscopically before IVF to improve success rates. In cases where tubal damage is too extensive for repair, IVF bypasses the tubes entirely and is very effective.
Pelvic adhesions are bands of scar tissue that form between pelvic organs — the uterus, ovaries, fallopian tubes, bladder, or bowel. They develop when the body's natural healing response to inflammation, infection, or surgery produces excessive fibrous tissue that sticks organs together.
Adhesions may cause no symptoms at all, or they may cause chronic pelvic pain, painful intercourse, or bowel-related symptoms. In terms of fertility, they can restrict the movement of the fallopian tubes, prevent the tube from picking up a released egg, and pull organs out of their normal position. Laparoscopy is the most reliable way to diagnose and treat adhesions simultaneously. During the procedure, adhesions are carefully cut and released, restoring normal anatomy as much as possible.
Pelvic inflammatory disease is an infection of the female reproductive organs — including the uterus, fallopian tubes, and ovaries. It is usually caused by bacteria, often spreading from the vagina or cervix upward into the pelvic organs. Sexually transmitted infections (STIs) such as chlamydia and gonorrhoea are common causes, though other bacteria can also be responsible.
PID can cause significant damage to the fallopian tubes. Even after the infection has been treated, scar tissue may remain inside and around the tubes, causing blockage or restricted movement. Repeated episodes of PID increase the risk of tubal damage substantially. Women who have had PID are at higher risk of ectopic pregnancy (where the embryo implants in the tube rather than the uterus) as well as difficulty conceiving. PID is a preventable and treatable cause of female infertility conditions, which is why early diagnosis matters so much.
PID is treated with a course of antibiotics — sometimes more than one type is needed to cover the range of bacteria that may be responsible. In severe cases or when an abscess has formed, hospital admission and intravenous antibiotics or surgery may be required. After treatment, Dr. Fathimunissa investigates whether any lasting damage to the tubes or pelvis has occurred and discusses the most appropriate fertility management plan based on the findings.
Endometriosis is a condition where tissue similar to the lining of the uterus (endometrium) grows outside the uterus — on the ovaries, fallopian tubes, pelvic lining, or bowel. This tissue responds to monthly hormonal changes just like the uterine lining: it thickens, breaks down, and bleeds. But unlike the uterine lining, it has nowhere to go, causing inflammation, scarring, and the formation of adhesions over time.
Endometriosis affects fertility in several ways. It can cause structural damage to the fallopian tubes and ovaries through scarring and adhesions. Endometriomas (cysts filled with old blood on the ovaries) can damage the ovarian reserve. The inflammatory environment in the pelvis can impair egg quality and embryo implantation. Endometriosis is one of the most significant and underdiagnosed female infertility conditions, often taking years to be properly identified.
Treatment depends on the severity of endometriosis and the woman's fertility goals. Laparoscopic surgery to remove or destroy endometriotic deposits and drain endometriomas can significantly improve fertility outcomes. For women trying to conceive, surgery followed by natural attempts or IUI may be recommended for mild to moderate disease. IVF offers good results for moderate to severe endometriosis, particularly when tubes or ovaries are involved. Hormonal suppression therapy controls symptoms but is not used during attempts to conceive. Dr. Fathimunissa takes a personalised approach, balancing symptom management with fertility preservation.
Sexual dysfunction in women refers to persistent problems with sexual response, desire, or comfort that cause distress and affect intimacy. While it is less often discussed in the context of fertility, it can directly reduce the frequency of intercourse and therefore the chances of natural conception.
If intercourse is painful, avoided, or physically not possible, natural conception becomes difficult or impossible. Vaginismus (involuntary muscle spasms that prevent penetration), dyspareunia (painful intercourse), or low libido can all reduce the opportunity for conception. These issues are more common than many women realise and are nothing to feel embarrassed about. Addressing them is simply part of a complete fertility assessment.
Treatment is highly individual and compassionate. Physical causes are addressed with appropriate medical or surgical management. Hormonal issues are corrected with targeted therapy. Psychological factors are best supported through counselling or sex therapy alongside medical care. Dr. Fathimunissa creates a safe, non-judgmental environment where women can speak openly about these concerns and receive the full support they need.
Recurrent pregnancy loss (RPL) is defined as two or more consecutive pregnancy losses before 20 weeks. It is a deeply distressing experience and one that deserves thorough investigation rather than simply being attributed to bad luck.
Each pregnancy loss carries its own grief. Recurrent loss compounds this significantly, affecting mental health, relationships, and a woman's confidence in her body. Beyond the emotional toll, it also indicates that something is either preventing the pregnancy from developing properly or causing the uterus to reject the pregnancy at a specific stage. Understanding why is essential to preventing it from happening again.
A thorough investigation includes blood tests (hormonal, immune, and clotting screens), uterine assessment with ultrasound or hysteroscopy, genetic karyotyping of both partners, and analysis of any available pregnancy tissue. Treatment depends entirely on the cause identified. Uterine abnormalities are corrected surgically. Antiphospholipid syndrome is managed with aspirin and heparin during pregnancy. Hormonal issues are treated with appropriate medication. Where no cause is found, supportive care with close monitoring from early pregnancy can improve outcomes. Preimplantation genetic testing (PGT-A) during IVF can screen embryos for chromosomal abnormalities before transfer.
Holistic fertility management means looking at the whole woman — not just a single diagnosis or a specific organ. It recognises that fertility is influenced by physical health, hormonal balance, emotional wellbeing, nutrition, and lifestyle, all working together.
Many women who come to Dr. Fathimunissa at Fatima Fertility Centre are dealing with more than one of the conditions described on this page. A woman may have both PCOS and a uterine fibroid. Another may have endometriosis alongside low ovarian reserve. When multiple factors are present, addressing only one of them gives incomplete results. Holistic management ensures that all contributing factors are identified and treated together — which typically leads to significantly better outcomes.
Holistic fertility management at Fatima Fertility Centre includes comprehensive hormonal profiling, nutritional assessment and dietary guidance, weight and lifestyle support, stress management advice, psychological support where needed, and coordination of medical or surgical treatments in the right sequence. Dr. Fathimunissa also ensures that any underlying health conditions — such as thyroid disorders, diabetes, or anaemia — are properly managed before and during fertility treatment. The goal is to bring the body into its best possible state before attempting conception, whether naturally or with assisted reproductive techniques.
Many female infertility conditions develop silently. A woman may have a uterine septum without any pain. She may have PCOS with only mildly irregular periods. Endometriosis can be present for years before it is identified. By the time a woman begins trying to conceive and realises something is wrong, valuable time may already have passed.
Early diagnosis changes outcomes. It expands the range of treatment options available. It protects ovarian reserve. It prevents conditions like PID or endometriosis from progressing and causing more damage. And it gives women the knowledge they need to make informed choices about their reproductive future.
If you have been trying to conceive for more than 12 months without success (or six months if you are over 35), or if you are experiencing symptoms such as painful periods, irregular cycles, or pelvic pain, seeking a specialist opinion now is the right step.
Dr. Fathimunissa at Fatima Fertility Centre, Chennai, provides thorough, individualised assessments for all female infertility conditions. Every consultation is handled with complete confidentiality, clinical expertise, and genuine care.
Meet our experienced team of anaesthesiologists dedicated to your safety and comfort
Take the first step toward parenthood. Book an appointment with our expert team to receive expert guidance, emotional support, and advanced fertility solutions designed just for you.